1. Many new nurses make the same or more and long time nurses. It's frustrating when the nurse in charge with the most experience is making less than new nurses. Some hospitals are even trying to stop nurses from talking about pay.
2. Patients in COVID have become downright mean. Add this to the problems nurses have management and doctors (who are often rude and arrogant) and it's a poor culture. The quality of the environment, from a mental health standpoint, is on the decline.
3. IT systems that they have to use were designed by people who have not talked with the workers who use them. They may have been designed with laws and compliance in mind. Nurses aren't the people who choose or pay for these systems. But, they use them a lot (maybe the most) and it's obvious they weren't taken into account when designing the UX. It's maddening for them.
This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
4. Nurses are the catch all for jobs. Not enough aides? Nurses do the work. Food service workers don't want to take food into a patients room... nurses will do it. Not only do they have higher ratios of patients but they fill in the work when other areas have shortages, too. So, the work per patient goes up. Pay doesn't go up, though.
Hospitals have made sure they hire JUST ENOUGH nurses to cover shifts and no more. With covid hitting, this blew out the number of nurses needed resulting in a lot of "I know you've already worked 60 hours, but can you do another 20? we are short!".
Rather than hiring permanent people or upping salary, Hospitals have instead elected to just use travel nurses and an extreme premium so as to avoid any salary increases.
The fix is one that Hospital admins don't want. Pay your nurses more and hire more than the minimum to cover shifts so a nurse being out sick doesn't result in another working a 80 hour week.
So, instead it's been day old pizza with superhero stickers.
5. Pay cuts - Most of the critical doctor specialties (ER, ICU, primary) that were the backbone of the pandemic got "raises" that were less than inflation (hers was 1.5%) while profitable elective specialties got big raises. The root cause is the billing system where elective surgeries bill pay out more than critical roles. Still, it's extremely demoralizing to be called a "pandemic hero" and have your pay get cut.
6. Criminal and Financial Liablity - Healthcare is delivered by a team yet the financial and criminal penalties for mistakes are assessed at the individual level. Recently a nurse was given a criminal sentence for a drug mistake which many believe was systematic failure (bad UI / IT systems, bad hospital practices, AND negligence on the nurse). Imagine getting sued or jail time as an engineer for dropping a production database. The few malpractice cases my partner has been involved in, it was very clear that the issues were systematic and perpetuated by hospital practices. However, if they had gone to trial, an arbitrary worked would d have been sued and the hospital wouldn't change its crappy practices. Institutions have effectively dodged liability in many cases.
7. Chronic understaffing and burnout - most ICUs have been understaffed throughout the pandemic. From an economics POV it seems crazy that their is a labor shortage but salaries are effectively dropping.
So...this is also the biggest reason (besides lack of pay or basic human dignity) that restaurants and retailers are having a lot more trouble finding employees. Rude (and sometimes violent) customers were already an issue, but they've become absolute animals lately. It's increasingly bad for your own health, mentally and physically, to have any public-facing job. In the last few years, we've let go any pretense of expecting people to be civil and reasonable, and adult children are rewarded for their behavior instead of being trespassed.
Teachers are also quitting in droves (and in the middle of the school year, in some cases) for the same reason. Children are awful and the parents are worse. You risk sickness and violence, and are constantly harassed by parents. Then there's the whole attack on the curricula and book banning...
The FAA reported 1099 incidents with unruly passengers last year, up from a normal 100-300 in prior years. Because some sorts of people simply won't do what they're told...and disobeying flight crew instructions is generally a federal crime.
Everyone's increasingly overworked and underpaid, and they have to deal with degenerates like that daily. Of course they want out.
We're having a societal implosion.
You're right that there are definitely opportunities for improvement here. As a Product person that has worked in EMR/Healthcare IT systems, I can tell you the biggest challenge is most of the decisions are driven by legally-required compliance. In many cases, you literally cannot make it better because the brokenness is /by design/ to comply with the law.
Nearly across the board, especially in the US, our legal and regulatory climate has not kept up with technology and often actively works to the detriment of technical innovation and improving our systems.
I think this is looking at the problem wrong. The problem is that implementing positive change in these systems is impossible for reasons far outside the control of any product designer or developer currently on the team.
This software is old, has byzantine requirements, probably cut costs all over the place, and conceived in a board room without the benefit of an adequate development lifecycle or stakeholders advocating for the users.
It probably takes 3 months to move a button around, and instead of moving that button executives are having them push a feature that earns a few more million, or a feature that the customers want more then a UX improvement.
Look at the RaDonda Vaught case or the Michelle Heughins case; terrifying to be looking at jail time for a med error.
Many nurses are watching these cases more closely and deciding that since staffing isn't getting any better and they won't be protected, it's not worth the risk.
[1]https://www.npr.org/sections/health-shots/2022/03/24/1088397...
There's no way to get a certification with online learning or with any kind of in person time schedule compatible with my job... ok... maybe I can get time off? I have to re-get all sorts of immunizations I already have and re-do medical checks that I already had to get for my green card, like a year ago... ok... that's a lot more time off. Oh, they drug check me! well... I guess even I would work on healthcare more for vocational reasons I'm not doing it while I'm in California. It's just too much of a hassle and with the staff shortages I feel I'm just being taken advantage off.
In Nevada it's only take the course, pass the exam and you can already go on an ambulance, so are most other states.
> This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
This resonates with me strongly for two reasons. First my mother is a retired RN, and the electronic record keeping was her biggest frustration. It is hilarious to me how much my mother hates computers, while I make a living in software.
Second, I'm now working for a startup, Smarter Dx (we're hiring: https://angel.co/company/smarterdx/jobs ) that works with these records and tries to make better use of them. To the extent that we're successful, incentives are created for the hospital to improve them, conceivably including improving the UX that nurses see. I don't mean to underestimate the difficulty of the problem, but I think it's possible to at least push in the right direction.
20 minutes later (while my mom was well on her way into work) the phone rang again- it was a false alarm, she didn't need to come in anymore. Naturally, it was my (not so happy) dad who answered.
By the time she got in, they didn't have anything for her, so sent her back home.
At the time, there wasn't quite such a crunch in nursing, so the pay part wasn't accurate yet, but everything else you listed (substitute COVID for %50+ of patients) was already true 30 years ago.
You couldn't be more right about that. Last week a nurse had to use a computer in my wife's hospital room to log that she'd given her a painkiller. The IT staff had failed to configure the hospital computers to disable windows updates or restrict them to off-hours and the nurse was forced to stand there for ten solid minutes while Update churned, the pc restarted, and Update churned some more.
I'd add to #1 that travel (temp) nurses are making 4x+ more than staff nurses, I've heard as high as $13-17k per week in high-demand areas. This exacerbates the problem, as staff nurses hear this, and if they can, they leave. Travel nurses can be great, but they won't know the facility and workflows and people as well as staff nurses: staff nurses now pick up more slack, all while getting paid 1/10th what their new colleagues are. This is more than most doctors.
For #3, this problem is made worse by additional compliance burden. Nurses need to document more and more, click more and more, read more and more… with less and less time. And on systems that are unpleasant to use. Among other issues, this leads to problems like these[0], which drive more and more nurses away.
I'm working with a badass team on solving some parts of these problems, particularly relating to technology and workflows. If you're interested (across basically any role, but product designers, engineers, product managers are top of mind right now), let me know (email in bio)!
[0]: https://www.cbsnews.com/news/radonda-vaught-nurse-guilty-dea...
I can speak to this a bit. After interviewing lots of hospital workers, I can tell you that the hospital quality people love EHRs because the reporting functions actually work. Previously, it was not possible to measure how well the hospital was doing and convince the doctors to improve practices - think washing hands before doing examinations.
EHRs are shitty because (1) the big players are entrenched - they are already implemented and the cost / disruption to switch to a new EHR is extremely high, and (2) the market isn’t big enough to justify the level of investment it will take to break through - Apple made more money from one product (AirPods) last year than all the EHR vendors combined.
At this point my hope is that mobile devices and meta-EHRs are able to crack this.
The nurses aides would argue that they do the majority of the frontline work while getting paid a fraction of what the nurses make, and get even less credit.
I think non-performance-based pay is something endemic to many female-dominated professions. My wife used to work in childcare, and it did her head in that she was paid less than complete idiots who'd been working there longer than she had.
- There is a ladder of nursing credentials, and the shortage effects them differently. Hiring for roles like CNA and LPN/LVN has exploded because of the shortage of RNs and above. CNAs get trained in 4-12 weeks to do the heavy lifting of care; RNs get ~3 year degrees to perform much more complicated tasks.
- Burnout, and the nursing shortage, are in a positive feedback loop/downward spiral. That is, the more nurses burn out, the more they cause other nurses to burn out. Short-staffed facilities have a very hard time pulling back to normal staffing, because nobody wants to join a skeleton crew. (I know of long-term care facilities where the scheduling nurses (the bosses) are working the graveyard shift because they can't fill it.)
- Many nurses work rigid schedules on 12-14 shifts, and a lot of medical errors happen at the end of those shifts. *
- The hot US job market (Great resignation, great reshuffle) is hitting nursing especially hard; it is very sensitive to external shocks. There are paths to easier work and higher pay.
- Many healthcare facilities and systems don't give nurses flexibility or the possibility of advancement. (One family member will need to quit her current job and come back in a year or two to her current employer if she wants to move up a pay grade -- which is like some tech companies -- but slower moving and lower paying.)
- Many facilities are run entirely on foreign staff (the H2-B visa allows that). And many nurses are imported from the Philippines.
* https://www.nursing.upenn.edu/nhhc/workforce-issues/where-di...
* https://www.nytimes.com/video/opinion/100000008158650/covid-...
(plug: if you're interested in this problem, we're hiring: https://culture.clipboardhealth.com)
(2) is a really perverse statistical phenomenon, and it's unfortunate that nurses are bearing the brunt of our civic and public information failures. It must be particularly soul-draining to heal someone who resents the single thing that would have protected them the most from needing hospitalization in the first place.
Pedantic, but: I think it's the responsibility of the people that pay for it to talk to the people who use it, and buy the best software.
I have a hard time believing that you can sit a bunch of nurses in a room to talk about the software, and that they'd design and/or elaborate on an awesome UX. Is there an example of that ever working? People have funny ideas about what they want. Homer Simpson's car design is a meme for a reason.
Maybe, but nurses have also used "because covid" as an excuse to engage in some pretty awful behavior. Fathers have only very recently been allowed in the room during ultrasounds, for instance. NICUs only recently started allowing both parents to visit at the same time.
It sounds like the issues nurses face are global and do not significantly change across different systems (the system in my country is completely different from USA)
It probably comes down to the fact that this is a human problem and to solve it we must radically change the expectations around care and primarily being taken care of.
There's no technological deus ex machina or amount of training that can change the situation without shifting the POV.
IMO people working in HC are subject to a lot of stress and must be protected at the cost of making it a bit unpleasant for the patients to be cured.
It's such a fundamental foundation of our lives that the system should be calibrated to create the best possible working environment for those who are working instead of moving it toward a customer reviewd activity that focuses on their satisfaction.
I know it can sound unpopular, but receiving the best medical care possible is not a right, it's a goal that more often than not it's almost impossible to achieve, so let's improve the working conditions so that the workers can give their best without questioning too much all the sacrifices that the job requires.
If you know ANYTHING about finance, that should send shivers up your back and also make you realize why this happening with nursing.
Private Equity is where you go to get money if:
• Your business is floundering and no one will loan to you
• Your industry is in the ebbing phase and not growing
• You are ignorant or naive about getting money for business
• You haven't done your due diligence
• Your company is in play for a hostile take-over
Having Private Equity getting involved is always a major Red Flag if not Black Flag.
In general, Private Equity knows nothing about your business norms or markets - they don't care. They are a one-size-fits-all investor and that primarily means "Cut Costs on Everything".
It's very akin to having a lawyer become your CEO (e.g. Sears/Kmart) - it's a omen of VERY BAD things being imminent.
A case in point: the COVID bounties from Medicare for testing, admissions, treatment AND DEATH BY COVID are exactly something that Private Equity would love maximally, dream up and probably try to enact with lobbyists.
This was exactly my experience when I worked for a medical software startup. Our (very unfinished) software got deployed in a hospital with no training, no orientation, no nothing, and it was such a disaster that it was a patient safety issue. Mind you, the engineering team had no say in any of this, not that we were even given the chance, and we weren't even aware that the deployment was for real. We were under the impression that the deployment was for testing purposes, because we were aware that the software was unfinished.
It was a breathtakingly poor decision purely on the part of managers (and, frankly, sales) on both sides of that deal and it was doctors and patients who suffered because of it. An absolute nightmare all around and I'm glad to no longer be there.
This!! I had a friend who retired early because she was literally being worked to death. A big part of that is the hours she spent after hours trying to deal with the new IT system.
Anyway, it's nice to make software like that :-)
>This one is big for product designers. Often we listen to the people who pay for it and miss out on the people who actually have to use it.
Thats an interesting comment because I know the main developer for one of the most popular hospital systems used throughout Europe and its popular because its good.
Saying that, I also know there are medical consultants at a world famous hospital who dont really know how to program but because of their position have got their software in use when it perhaps shouldnt be.
I know alot of US programmers doing various medical systems for local hospitals and health care regions with various standards of programming skills.
Like you I also know of people in various roles, from world famous multi millionaire consultants to nurses on the front line. Every team & dept is different. Sometimes its a managerial problem at the top of the health trust, other times its just the team and low level management.
Saying that there is a culture of taking a sicky probably because they see consultants putting private work before NHS work and they see the wages some of these consultants get paid and Google Scholar, PubMed, DrugBank etc keeps highlighting the inadequacies of the teaching, ie they dont keep up to date, some areas appear to be decades behind the science other areas are within a few years of the latest research.
Too much reliance on drug companies when superior non patentable solutions already exist.
Interesting thread because this is my current $dayjob! I work for an organization that is both a tech company, and a medical services provider, so we can optimize away the boundary between vendor and customer as far as the software is concerned. My particular area of interest is in providing system programmability that can be exploited by tech-capable clinicians to provide both better patient outcomes and more pleasant provider experience. Basically don't try to have software developers understand every last detail of the practice of medicine. Instead provide a programable platform that's usable by a subset of clinicians.
Ultimately, it is not the radiologists or technologists who make this decision. From a purely technical point of view, modern systems hardly differ from each other, at least as far as diagnosis is concerned. The fact that a better UX means new users need less training and the time between scan and diagnosis is reduced are hardly taken into account when making a purchase decision.
Every time the computers went down at a friends ER, the waiting room emptied out as the staff were able to use paper forms and just get their jobs done, instead of being forced through thousands of menu clicks and choices that made no sense.
EVERY SINGLE TIME -- Epic or as I call it... the Epic Failure. I always give my condolences to staff forced to use it.
No idea where you live but in German hospitals I've never been given the food by anyone but a nurse. There are literally zero people/professions besides doctors, nurses, and cleaning staff near patient rooms.
I worked at a large emr company and the developers had access to nurses and were required to support go lives a few times a year to support nurses on the floor.
This is a very common issue with enterprise systems, since incentives aren't aligned. Users of such systems aren't the ones choosing them.
I wonder if you are talking about Eclipse software which seems to be universally frustrating for doctors and nurses across many countries.
Is it mainly lack of information (and exhaustion) that prevents these more experienced nurses from negotiating for what they're worth?
My mom worked in food service for several years at a hospital and took the food into the rooms. Is this not the norm?
For profit healthcare is an abomination and a blight on the very soul of this country. If I believed in religion I would say God will judge us very harshly for allowing this system to stay in place for so long.
Working in Healthcare IT I can only concur on this point.
For me there's multiple reasons behind this issue :
1. Regulations. First and foremost, IT is here to help/force users in complying to those regulations. So it's the first thing that dictates how you'll develop the piece of software. Those regulations are mostly written by people that aren't Healthcare professionals nor IT professionals. They are regulations people. So they can't produce something that makes sense for Healthcare people and is even harder to _solve_ for IT people. And those regulations are updated quite frequently, most often creating breaking changes. So if you want to keep up (and you have to if you don't want people ending in jail) you must work fast, meaning skipping important steps to produce something user oriented.
2. There isn't much money. At least on my side of the Atlantic. This is not necessarily a huge problem because contrary to people at FAANG-like companies, here most people are focused on helping people to help other people, not on their paycheck. But there's so much middle-men taking their cut that in the end, you only worked understaffed with unrealistic schedules. Meaning the only way to deliver something is to take big shortcuts. And again, leaving UX/UI on the side of the road to reach the main goal : being compliant with regulations. And when I say there isn't much money, it's partially true. When it's about buying a nice startup, there is heaps of cash. Because you need to keep the market as closed as possible. But when it's time to actually invest in making better software, the wallet is empty.
3. There's a weird mindset where in most cases, end-users are simply not considered. At my previous jobs, I always asked to sit with actual users of the software to see how they work and what their actual requirements are. Since I joined Healthcare IT, on the ~20 projects I worked on, there's only one case where I was authorized to do so. On all the other cases, the "IT Project Manager" (whatever this is) just said that they knew exactly what the users needed, even though they never actually worked with them. And on the project I was allowed to work correctly, instead of the original proposal that was agreed on, based on my observations, I came up with a solution that was much simpler for the users, easier to build for the IT team, so delivered faster and at a lower cost. So the customer was happy and decided to sign a contract for another piece of software at the company. Everyone happy in the end. But it's an exception. In the other domains I worked on, it seems obvious to everyone that gathering intel from the actual users was mandatory to produce something valuable. Here, management think they know better. They don't.
And honestly I don't see how it can improve since those three points keep getting worse and worse every half-year.
Mean customers, and rude coworkers? I sympathize, but this is a reality in a lot of industries. I have no reason to believe that healthcare here is worse than average.
I think a computer guided system would help. My experience in lower grades, high school, college and grad school is that there is a consistent lack of showing students the concept of self-study, this is exemplified with the famous self studiers AKA autodidacts, like Newton as a prime example. This skill is a very important one to develop early in children. Sort of give a person a fish a day - or teach him how to fish. Online teaching at all levels up to and perhaps including grad school is well suited to complex programs that show a student a module of this or that. This can be history or mechanics. After the module is presented, the student is queried on the facts of the lesson and then asked what he can deduce from the lesson. Say the 300 against the Persians - why did the Persians fail? The student should then deduce that because the front of battle was only 30 people wide that it was a battle of 30 against 30, and better training, armor, skill and weapons that meant the Persian masses were useless - it was an attritive war of 30:30 until one side lost enough men that it became 30:29, 30:28....30:1 = war over. Some students have greater intelligence and will analyze this aspect correctly. Those that do not are sent to the first fork..... and on to the full analysis. In this case, the Greek better arms/skills may well have endured until the entire 300,000 Persians were killed, via re-supply from various Greek city-states - in this case, the Persians did an end run and were able to change the combat ratio to the point where the Greeks were overwhelmed.
Going to the general case:- The auto-didactic skill of the student needs to be developed one-on-one via the skillful design of the course material, with forks and subforks and re-entrant forks into the stream as each student masters an item and proceeds. At every point there should be a fork for every fail point - you can have as many forks as needed to imbue understanding. Modern computer systems are quite capable of this degree of complex interaction - but it requires a good amount of work with both masters in topics(many of them to variegate the forks) and up to now I have seen few produced. Large amounts of $$ and time have been spent on thousands of parallel minimalist approaches - it needs a central command/fund structure. /rant...
- Demanding work: 12 hour shifts, irregular schedules, night shifts, physically exhausting, limited breaks (including bathroom/water!)
- High responsibility with unsafe conditions. You're literally responsible for people's lives. Poor staffing ratios stretch you thin and make you more likely to make mistakes. And if you make a mistake, you're at huge risk for litigation... and now criminal consequences too. Responsibilities, resources, and staffing stretched even thinner due to the pandemic.
- Administration that treats you as something to be optimized and does the absolute bare minimum to support you. Instead they tack on additional tasks, expectations, and requirements ("no water at a nurse's station!"). They encourage a culture where nurses provide a concierge service to 'guests' instead of critical care to patients.
- Hostile/entitled patients. I'd guess many/most patients are not an issue, but it only takes a couple of difficult/combative patients to really ruin your conditions.
- Low pay given the responsibility and working conditions for non-travel nurses. https://nurseslabs.com/nurse-salary/#nurse_salaries_by_state Like many others pointed out here, in tech I make way more than a nurse for a job that's less demanding, has far lower stakes, and is of far less value to society.
To me the blame lies mainly in middle/upper management, whose role is to build and empower an effective workforce. If 90% of your workers are considering leaving, you blew it.
Nurse: It's really hard for us to hold on to our good nurses, we can't afford support staff so they get stressed out and leave for traveling gigs.
Me: Why can't you afford support staff?
Nurse: The traveling nurses cost 3x more. We have to hire traveling nurses to replace the ones that left for traveling gigs.
Me: ...
Nurse: I know...
Me: Can't we just... pretend they are all traveling nurses?
Nurse: I know...
I'm not a big fan of defrauding your employer, but sort of hope that some of these "traveling nurses" are somehow swapping gigs secretly and subletting their temporary housing to college students.
The pay to responsibility ratio for nurses is absurdly low. So unfortunate given the difficulty of the profession. I guess we'll see if anything changes over the next handful of years.
Sometimes, it feels like we’re min-maxing ourselves to death over here.
I knew of certain defunct malls that decided to get rid of things that doesn't make money and only keep the high profit inventories.
Soon people stopped coming and they went under..
The first, mentioned already in this thread, is that maximizing profits should not be the ultimate yardstick in all cases.
The second is that we are not setting incentives correctly in healthcare: preventative care still plays second fiddle to curative care. If the healthcare industry were purely free market, this could be attributed to individuals not understanding the long-term benefits of preventative care, or overly discounting the distant future. But the healthcare system is not purely free market. The largest payers, public and private, could do a lot to correct the incentives by setting their reimbursements accordingly.
I hate every part of it.
The WWII generation fixed the ozone hole, but their kids didn’t lift a finger for global warming.
Subsequent generations are scrambling to pick up the pieces for our kids, while crap like this, and our rapidly collapsing democracy keep sabotaging our efforts. Heck, in California, we’re actively causing psychological harm to an entire generation of kids (with masks) because of a tiny minority of anti-vaxxer school teachers.
Of course, progressive boomers exist, as do idiotic younger people. However, the current generation of leadership in the US has completely failed us.
Anyway, it’s not surprising to me that that crowd decided to shunt healthcare resources away from their (great) grandkids and into elder care.
If it's entire purpose was to provide pediatric healthcare it should probably have registered itself as a not-for-profit.
I feel like a waitress, custodian, social worker, therapist, punching bag and other stuff - It's never ending. This has effected my mental health so much that I am slowly doing my career switch to SWE. While I know every job has it's own difficulties bs/stress/politics, the one's i deal with as a nurse now I can no longer deal with. I don't regret this career path because it has taught me a lot, and their is something better for me out there.
Career: I did consider other areas of nursing, but they didn't satisfy me, ICU is relatively the most enjoyable for me. On a regular hospital floor/intermediate floor, a nurse will be given 4-5 patients and let me tell you its a ZOO! In ICU i only have 2, and those keep you busy the whole shift. They're both different kinds of crazy.
I will say, being a nurse in California is 5x better than anywhere else simply because their are laws that allow us to have uninterrupted breaks!
I just wanted to say that it’s a sad state of affairs when we’re happy to expect uninterrupted breaks. Goes to show just how much we _really_ supported our frontline workers.
Best of luck to you!
Outside of the existing issues with Bedside nursing (long days, physically demanding) - the primary issue is staffing. Pre-pandemic the ratios were already bad but now many are leaving for travel contracts which carry significantly better wages. It quickly becomes a loop where employees leave for Travel Contracts, and then can only be backfilled with Travel Contracts. The remaining FT staff nurses are left making much less money, and have to assist "training" with the outside Travel nurses. And while this is nothing against them - The travel RNs also often have a different "vibe" as they are much less focused on long term improvement or problem solving within the Unit.
Also ICU/PCU/ER nursing throughout the pandemic was a terribly depressing place to be. Leaving many of my Wifes colleagues (including herself) with what is essentially PTSD with little or no support from the Hospital System.
We are talking about the people who clean up the nastiest human waste that our bodies are capable of producing. I was already surprised that this number was ever less than 100% tbh
If you’d cut your pay down to 25% of what you make, work 12h a day with a single 30min lunch break (that gets interrupted regularly), including several weekends and nights every month, without guaranteed vacations for holiday season/new year’s eve, work in a team that’s 50% understaff but still needs to deliver no matter what, without any carrer path forward, you’d leave your current SWE job right away. And in comparison, you’d still not be be even to close to what they do (i.e: cleaning up body fluids).
More importantly, a lot of them will be leaving though burnout and depression (a significant number of hospital staff is already on this course).
From my perspective, the entire healthcare industry is set up to treat any frontline worker without an MD after their name as completely expendable, nothing more than a row in a spreadsheet that can be optimized for middle management to hit next quarter's bonus targets.
You can meet all metrics management sets out for you, have amazing patient satisfaction scores, etc, and every 6 months some spreadsheet wielding online MBA graduate is going to show up to turn the screws and tell you you need to work harder for the same pay, and to just be happy you aren't getting laid off.
At some point in time, the workers realize the joke is on them and find another profession.
here are some "articles" on the subject:
https://www.bmj.com/content/373/bmj.n1594
https://www.beckersasc.com/benchmarking/22-of-physicians-con...
https://www.medpagetoday.com/practicemanagement/practicemana...
And one of these articles (the last) is from 2013, talking about a change in healthcare practices (corporate unification), the ACA (limits on accepting medicare patients) and the health reform law (liability reform). So, I guess medical burnout has been coming log before Covid and we have just been ignoring it?
I was at my family's Easter lunch last week and one of my uncles who's an MD was telling me about the mass exodus of doctors from the profession since COVID hit. Anyone who was thinking about retiring did so once the pandemic took off.
He then tried to convince me that I'm not too old to go to medical school. Yeah, no thanks.
By the end she was seeing twice as many patients a day as before with no time to do admin stuff at work even after skipping her lunch break so she also had to do more work when she got home. The reward for doing double the work as before? A 10% pay increase barely above inflation. Meanwhile a few coworkers left and no new ones were hired so the workload just kept increasing.
It puts providers in such a bad position because the only way to push back is to drop the level of care, which has real human consequences.
1. Safe mandated staffing ratios. California is one that does this and many nurses seem happy with the ratios.
2. Safe harbor laws. If the nurse feels they are pushed into a risky situation, they should have a right to notify management which will take on liability if they do not resolve it. A few states have this but hospitals bully nurses not to invoking it.
3. Better pay for the liability they take. Unlike management, they could go to prison for mistakes they make. There was a recent case nurses were outraged about.
4. Unions are beneficial. In California the nurses union is pretty strong to negotiate better terms and conditions.
The nursing crisis is 57 years old now: https://pubmed.ncbi.nlm.nih.gov/14252064/ (1965)
Similar articles
WHY THE NURSING SHORTAGE PERSISTS.
HALE T. N Engl J Med. 1964 May 21;270:1092-7. doi: 10.1056/NEJM196405212702105. PMID: 14121489 No abstract available.
STUDENTS' DISAPPOINTMENTS IN PUBLIC HEALTH NURSING.
HANSEN AC, THOMAS DB. Nurs Outlook. 1965 May;13:68-72. PMID: 14291737 No abstract available.[0] https://trends.google.com/trends/explore?date=all&geo=US&q=n... [1] https://trends.google.com/trends/explore?date=all&geo=US&q=n... [2] https://trends.google.com/trends/explore?date=all&geo=US&q=n... [3] https://trends.google.com/trends/explore?date=all&geo=US&q=n...
Nursing is a well paying middle-class job without a lot of transferable skills to other professions. Don't say programming. It isn't the solution to everything. Other low-entry-barrier jobs pay much less and have exploitation problems of their own. For a lot of middle class families, dual income is essential to maintain their lifestyle. So SAHM is not an option. Nursing has clearly gone through a rough 2 years, but I suspect that things are going back to normal now. Why leave now ?
> High patient-to-nurse staffing ratios
This bit is confusing me. If supply-demand is in the Nurse's favor, then don't they get more leverage on what QOL and wages they can demand ? It is not like they can fire a senior nurse on low pay, when new nurses are harder to find and demand higher wages. I know that the nurses refusing work and resulting deaths has bad optics, but it doesn't look like hospitals have a lot of leverage right now.
> Administrative burden and manual tasks
Sounds like an opportunity for a startup to disrupt the space. But, the jaded side of me thinks that the startup will fail due to insufficient political leverage with hospitals/insurance/law-makers.
> health IT
Keep calling it health IT and the problems will never be solved. Solving hard problems needs reframing of the resources dedicated to it. When tech workers are seen as assets and not cost-centers, these problems will solve themselves.
I have a family member who works in public health and is trying to staff nursing positions. She has something like a $400k budget to hire 4 nurses at $100k each (let's say). She is unable to fill the positions because cost of living in her area has gone up so much. She'd rather have 2 nurses at $200k each instead of zero nurses, but she's simply not allowed to do that. She's trying to change policy but it's a massive uphill battle.
Power's concentrated very high up in health care, and it's exercised through the use of rigid policies. It certainly seems like nurses should command higher wages, but the bureaucracy has become very effective at preventing basically anything from changing quickly.
When we got married, my wife (Physicians Assistant) made handily more than I did. $140k to my $82k midwest, software development job.
10 years later, she makes $130k (after cutting hours back) and I make $4-500k as a software engineer in the midwest. The two markets crossed drastically
Where are they going?
For us, home.
Only in a vaccuum. It pays far worse than other jobs at the same rate given the effort and stress the job entails.
> don't they get more leverage on what QOL and wages they can demand ?
Sure, but it needs to get far worse. The hospitals are only going to budge once walkouts are organized. But that can't happen without strong unions, most nurses just need to pay the bills which is why they continue to put up with it.
I'm not sure you understand who has the leverage. The hospitals can let healthcare deteriorate far beyond current expectations. They still get paid in the end. The environment for patients and nurses will only get worse.
[1] The labor participation and employment rates for military spouses (especially when adjusted for age and education) are so low that they're almost off the charts. The causes are frequent cross-country moves to economically struggling locations, and an extreme need for flexible schedules (e.g. for when service members get deployed and spouses become de facto single parents). Medicine seems to be unique in that it's everywhere, always hiring, and often allows for part-time employment.
Whelp, that the whole point. When you have a good paying job and people are leaving in droves for ??? anything else, maybe even teaching or staying home. That's a bad sign.
I have many friends and relatives that are nurses, MDs, and therapists.
Compensation is about as backwards as you can get. Seniority has no impact on your pay. Once you hit the ceiling you’ll never make more money. This is especially true for Nurses and therapists. Even if you switch jobs. The market rate is what you’re going to get paid (within 10%).
My wife is a PT and made 3x more traveling as a contract therapist than she did as a full time employee. Three times. That’s absolutely absurd.
Benefits are also beyond comical. Healthcare insurance costs for healthcare workers are higher and the benefits are worse than if you just bought Obamacare directly.
Beyond horrible pay with no upward mobility, you’ll also have to deal with completely disconnected management that has never done any clinical work in their lives. They’ll bitch and moan about saving money, and often enforce policies that put clinicians at risk of malpractice. All to save money.
So yeah. If I were to give any young people advice, it would be to stay as far away from healthcare as you can.
Self-insurance seems pretty common anymore. Which amounts to - you can receive treatment in the hospital you work in. You'd at least think it would at least be free, but nope.
- "Almost HALF Of San Francisco Residents Considering Leaving City" (according to survey of 500)
- "One in three New Yorkers Considering Leaving The State"
- "Over Half Of Young Lawyers Considering Quitting by 2027, IBA Report."
Look for X people considering Y, and you'll find them. Considering is cheap.
The awful experience of nurses, absolutely, true. But this, like so many others, is a silly poll that doesn't say anything.
A lot of people did leave NYC, and probably NYS. So if a much larger number than usual are considering leaving <fill-in-the-blank>, chances are that a larger number than usual will leave <fill-in-the-blank>.
But this sounds like the employee satisfaction corollary to Sturgeon’s Law [1].
“90% of employed people are considering leaving their profession in the next year.”
This survey would be more compelling if it compared nurses responses with the general employed population over time. I only skimmed so maybe it does and I missed it.
This was generally the case prior to pandemic due to how poor the work environment has become, but the pandemic seems to have broken the few remaining folks who still had hopes and dreams.
How doctors of all professions lost their professional agency to do-nothing administrators within a generation is quite puzzling and a bit terrifying to me.
Until I saw hospital nursing, I had never seen a company run by HR.
Every decision starts and ends with HR. From hiring, to wages, to discipline and promotion, to IT and pay-roll, to reorganization and spending priorities, there is a rule for that. Maybe that rule originally came from the CEO or the CNO, but they say things like "may" and get interpreted as "shall" (or the manager faces a bad review and/or termination) or they are interpreted beyond any rational meaning. My best explanation is that it comes from a fear of litigation and a lack of leadership at the top. The final hilarious story is the CEO negotiating a big deal with lawyers and VPs shaking hands... and then saying without joking, "but I'll have to get HR's approval". The meeting wasn't important enough for HR to show up, but they had the last say.
I have a lot of friends at various levels of healthcare, from nursing up through low and mid-level administrative positions.
The one thing they all seem to agree on is that patient satisfaction surveys have been terrible for healthcare.
Once the emphasis shifted to patient satisfaction, everything became more of a game of catering to what the patient thinks they want. With the spread of rampant medical misinformation on the internet and the rise of alternative-medicine podcasts/blogs/influencers masquerading as informed medical professionals they have a constant influx of patients who show up believing they have a certain condition or need a certain medication. If you disagree too much or refuse to give them the medication they want, you risk a negative review. Too many negative reviews could negatively impact your compensation or even cost you your job.
Even at offices that don't perform patient satisfaction surveys, providers are at the mercy of negative online reviews. Again, if you don't do exactly what the patient thinks they want, you risk scathing online reviews.
This is terrifyingly problematic given the trend of people to self-diagnose with anxiety or infections who show up demanding Xanax or antibiotics. Puts doctors in a situation where they don't really think prescribing those medications is a good idea, but they also feel like they can't deny too many patients or they risk their reputation/bonus/reviews.
It's also a huge problem with conditions like obesity or alcoholism or smoking, where the doctors can see obvious patient-induced health issues but the patient really doesn't want to hear the truth from their doctor.
You just summarized the decline of Western civilization in one phrase.
This has happened almost everywhere and efforts to push back have proven extremely difficult. I personally place a lot of the blame on the educational system for overproducing administrative skill sets and underproducing practical skill sets. There is some role for those things of course but we have far too many people for the administrative roles we really need and far too few for many other professions. This combined with the tendency of people to recruit people like themselves has oversaturated the market with administrators looking for reasons to exist.
The rot is to the point that we have the spectacle of Elon Musk looking like superman. Why does he look like superman? Because he actually does things instead of having meetings to discuss the meeting schedule. He's just a reasonably competent engineer and business founder with huge resources who... does things... and this makes him look superhuman by comparison to the hordes of administrators that only discuss doing things and commission studies about hypothetically doing things.
I would bet it's caused by:
- stifling bureaucracy
- hostile legal climate
- massive start up costs
The only winning move is not to play. Let the system fall apart and join on the later upswing. The unfortunate part is all the needless suffering people will endure during this process.
My mother switched to an administrative role internally, 10 years before she got retired and my sister went from nurse to anesthetist and now in the progress of moving to IT as a domain expert for medical software so she can work from home.
This should terrify everyone. Large segments of our society are failing us despite being stuffed to the gills with administrative staff that don't contribute much to productivity but rob professions of their independence. We're managing ourselves to death.
My mom was a long-retired medical director of a hospital and even she was shocked at poor quality of care, compassion and competence. Even in the ER of a recognized trauma center, things were pretty meh. Some specialist floors and ICU were good, but when an infection caused by poor hospital hygiene struck, he was relegated to the “medical” floor, where he was not fed, medicated, turned or treated with respect. Ultimately we maintained a 24x7 staffing of family volunteers for over 6 weeks.
Many of the staff frankly sucked. But it was easy to see why - the staffing levels were so poor pre-COVID, that any RN risks license every day by virtue of being there. The smart ones GTFO. You can’t care for 15 patients.
I’m pretty sure both of these will implode under the bureaucratic weight at some point — the financial and social costs of the excessive administrators is not justified by their (often minimal or negative) value added.
In my experience, the administrators are often doctors at hospitals and people all the way to the top have to have strong medical backgrounds. That's not to say there aren't do-nothing administrators, but those do-nothing administrators are often doctors. They tend to adhere to the way things are and always were as an orthodoxy, like 1st year residency is the worst and at these points quality of life improve, but it's almost like a fraternity hazing justifying the insane hours, complete loss of work life balance just because this is how it is. Candidly, there does seem to be a guilty pleasure there.
There is little to no real discussion on how to improve not only the work conditions but also the user experience of medical care. In my view, it starts at the top; organizationally, they are lacking an entire skillset to make any improvements what-so-ever.
Everything is controlled by insurance companies. You can’t do anything unless it’s exactly how insurance wants and only for what insurance will pay.
It limits everything, including how every profession can be compensated simply because you can’t easily hire somebody for more than what insurance will pay for their services. You can, but the funds have to come from somewhere.
She's looking to switch jobs now and her first offer expected her to travel to locations deep in queens, manhattan and brooklyn, seeing on average 50 patients a day. She currently works at one of the largest hospital chains in NY and is now negotiating an offer from the other largest chain, initially she was told to not worry about salary and that they'd be able to match her previous offer, then HR called her and told her she had 1 and not 2 years of experience so the best offer they can offer her is lower than expected, she said she wouldn't be able to do it so the HR people went to check again to see what they can do and it turns out they called up the hospital that my SO works at now and checked their pay tiers and said they can only match the number that they were told. The new position was close to where we live so she considered taking it anyways but they just called her again and asked her if she'd be willing to travel to other locations multiple times a week to help fill in gaps (but weren't even able to tell her which locations before accepting the offer).
TLDR: don't let your friends and family go into healthcare
Turned a "trusted professional" advisory role into a keyboard role.
Same thing with professors.
One of their neighbors used to work for a home healthcare company in the area.
Is it?
The financialization of every aspect of life, in this case with for-profit hospitals through multiple layers of insurance middle-men, the exodus you describe would seem one of the natural byproducts from miles away.
The profit model of the U.S. healthcare industry might have something to do with it. The fact that hospitals are run like businesses and have shareholders is insane to me. I know other countries' healthcare systems got hit hard by the pandemic too, but it seems like the uniquely capitalist nature of healthcare in the U.S. sets it up to mistreat workers and cut corners for the benefit of administrators and executives.
I wish I had more access to nurses during the process. I was always told they were too busy. I just wanted to observe, as I do with any client I write systems for, and was denied. I can say that at least 2 other groups were working on the exact same project as I in the hospital system, and we "won". We all worked in isolation from one another, I discovered the others by accident.
The top of major healthcare systems is wasteful and full of "little kingdoms". The ideas that "AI is going to help" and "nurses need to feel heard" are basically incompatible. Throwing money at artificial brains is always to substitute real ones, and the concept itself is contradictory to employee development. Why train a bunch of nurses endlessly on a subject when you can train an AI once?
We're supposed to be improving & developing people's lives here, not improving a box. For centuries we've found new ways of thinking that have made us better at science and medicine. Computers could do that, but we're not using them to teach each other. We're using them to replace one another.
It may sound silly, but I've reached the point that the theory Dune puts forth seems right.
But yeah, in general, this is a problem (healthcare in general, healthcare expenses, nurse job experience) where almost all other countries with similar wealth are doing so much better than us, it shouldn't be that mysterious to solve it, right? It's not like, who knows if it's even possible to do better! Like, we know it is... figuring out what the difference between them and us isn't trivial, but it should be easier than something there isn't a model for.
The most obvious difference would seem to be how insurance (and universal coverage thereof) is handled.
sqrt((p*(1-p)/n)
sqrt((0.9*0.1)/200) = 0.021
So 95% confidence interval for this ~ 0.86 - 0.94
Does that radically change the message of this article?
"I plan on quitting my job if I had money" wow stop the presses.
The deaths were always hard when working with little kids - and there were a couple a month. But towards the end of COVID they were losing 4 kids PER WEEK (anecdote - I have no data other than listening to them vent) that this nurse firmly believed were avoidable had they received appropriate care.
What caused them to exit was how the hospital handled COVID: they postponed all elective surgeries. For these children, an elective surgery was anything where they "wouldn't die tomorrow" if the surgery wasn't done (somewhat of an oversimplification - but ballpark correct).
During that time hearts got worse, cancer progressed, bodies shut down until electives became emergencies... Success rates of surgeries dropped. And once restrictions started lifting the staff was underwater, they had a huge backlog of "electives" piled up on top of the normal ingress - kids were dying from waiting.
Considering it was bothersome for both healthcare workers and the public, in my opinion the friction is more between the healthcare workers and management/government entities (& their policies) rather than "some patient bothered me" cases.
I guess my point is, not only is the current healthcare labor market at stake, but hiring/pay/working conditions now are having upstream impacts on the labor pipeline of people coming into the market, or evaluating entering healthcare. Having recently gone to the ER with my toddler, I can tell you this is not an area you want the market going for lowest bidder when you do have to use healthcare services.
They pride themselves in it being so hard instead of realizing that this is glaring problem that needs to be solved instead of nurtured.
This begins from medschool being prohibitively hard, to a lack of global licensing process, to doctors being on duty for 36+hrs when you cant legally drive a truck without stopping after 8hrs.
Its all wrong at every level.
And truckers are being abused in similar ways.
So hospital administration will have a fresh crop of graduates, new to the system, to abuse. The cycle will continue unabated.
I make slight improvements to computer systems. In most of the jobs I've done, despite my best efforts to work for reasonably ethical companies, I've not been convinced I've made anyone's lives better. Yet my salary is 2-3 times hers.
I find it hard to believe there can't be a better way to arrange this kind of stuff.
Even in the (US) medical system, pay/insurance reimbursement is based on the number of procedures you do, not how involved the treatment is. This is why surgeons get paid so much more.
1. Hire more nurses to spread the load around
2. Pay existing nurses more
3. Incentivize people to get the technical training required to become a nurse.
"But what about my boss's 4th home?" I know. I am worried about that too. i pay 1500/mo to live there, and the costs will probably trickle down to me. we will have to figure something out.
"But we don't have the money! Who is going to pay for it?" Well. Then I guess the goose is cooked. We no longer have the resources to run a functioning society. I want you to think about that, and maybe think if we could get the funding from somewhere.
We are out of trained workers. The money diet our overlords put us on has officially starved us. Welcome to the 3rd world. Hope you saved up enough money for a ticket to Elysium.
Nobody wants to take out student loan debt anymore. If you are over 30, let me fill you in: cost of college has gotten even more insane than when we were in school.
we are seeing the same thing in our courts. Everyone is mad at the PDX DA for turning people loose all the time, but the secret is: there are not enough public defenders, and we can't hold people indefinitely without cause. There are literally not enough lawyers graduating from law school/graduated in the past to fill these spots.
Our society is falling apart and all anyone can talk about is how lazy the homeless are and obsess over what genitals people are born with.
Absolutely! Thanks, this made me laugh out loud. It's almost as if the people in charge of society don't have the same interests as the rest of us..
The reason why, at least for that doctor, wasn't really the stress from patients. It was all the damned paperwork and the stress that created.
One of the PTs I know spent at least as much time filling out paperwork as he did with patients. This was partly due to the volume of paperwork required by govt / insurance / lawyers / whatever, and partly due to absolutely awful software.
He was admittedly older and had never particularly embraced computers and so forth.
(And then my new PCP retired during the pandemic.)
1. A few doctors left practices after they got taken over by a bigger entity and the hoops they had to jump trough weren't worth it, so they retired.
2. The insurance companies - they control EVERYTHING. One thing that happens a lot is that they don't allow her to order an MRI unless she orders an X-Ray first - even if what they're testing for wouldn't show up on an X-Ray. And this slows down the process of diagnosis by days. There are more examples of things like this - things that should be up to the provider, but end up being up to the insurance company (what drug to prescribe or what treatment to pursue first) - it makes no sense (at least from what I hear from her).
FHIR would be a good idea, but in practice its hard to correlate a patient across the systems. Few hospitals and doctors setup a push notification for when they change a patient's record.
Essentially all of the software needs to be redone with a focus on a centralized record tracking system. The rewrite needs practitioners (all of them, not just Docs, but the lowly CNA too) to drive the requirements. Admins should be included, but not the target of day to day UI.
So pay isn't the problem.
The U.S. is also above the OECD average for the number of nurses per 1000 population: https://www.researchgate.net/publication/334515420/figure/fi...
So staffing isn't the problem either.
The U.S. is below the OECD average for the number of doctors per 1000 population: https://www.nurses.co.uk/Images/Blog/media/ddad9fa9-b06d-43d...
If nurses could work a regular 40 hours a week and be paid more, as they would like, the additional money and staffing need to come from somewhere. In the United States, we've decided that private hospitals could have the right to exist. Most nurses are thus beholden to a free market. So the question is why other hospitals aren't trying to poach nurses with better wages and schedules. The reason may be that the supply of nurses remains large enough that hospitals don't feel pressured to make these concessions. The business model of hospitals is also drastically different from that of, e.g., tech companies. Tech companies can afford to pay their employees outrageous salaries because it is possible for one software engineer to create a product that will generate $100M in revenue. A nurse's labor has a cap on how much economic value it can generate. Hence why nursing salaries are constrained.
Do you think when someone evaluates if they're paid enough they're thinking 'what is my income relative to what someone else's income is in Belgium relative to other people in Belgium?'
Also, it looks like the outrageous costs of healthcare in the US don't correlate at all with nurses' wages. If I were a nurse, I would feel demoralised if I was doing a lot of the hard work, yet administrators and middlemen still get the most money.
Most nurses work three 12 hour shifts and are paid for 40. It's so prevalent that a lot of them will pick up an extra shift or two at an entirely different hospital.
You don't have enough data to determine that as you are assuming that the staffing levels should be the same between countries when due to things like a huge push to increase profits, more paperwork, and other such things they can be drastically different.
Or pay is a problem elsewhere too.
USA healthcare pretty broken, and sliding into catastrophe. Nurse dissatisfaction is just the tip of the iceberg, or the canary in the coalmine.
> Eighty-four percent of emergency room nurses and 96% of intensive care or critical care nurses have a 4:1 ratio, which is double the optimal target of 2:1.
> Thirty-six percent of nurses said they've seen patients with acute health conditions walk out of the ER because of the wait times for an inpatient bed. And 37% said that surgeries had to be rescheduled because of bed shortages.
In fact the entire website is probably a PR plant.
It's super, duper complex with lots of paperwork. The complexity is too great to run a small practice, the Medicare/Medicaid fees are too small to make up for it, and it increases the importance of administrators in the hospital system.
If I had a bunch of time I'd love to go through and write up a proposed alternative approach, and congressional bill -- but I have to imagine even if I did that, no one would listen to it.
This is an orphan statistic. What percentage of nurses considered leaving every year five years ago? Ten? Twenty?
It is also partly because the number of patients is increasing disproportionately, mostly because people are getting older. An individual at the age of 50 needed fewer medical appointments than an individual at the age of 70. That's literally from 2002 to today.
There just aren't enough nurses and doctors to tend to such a large old population.
This survey has such a low number of responses to make any meaningful conclusion from. 200 people surveyed. Non surprising stats like 71% of respondents having 15+ years of experience wanting to quit.
What really should be the lesson here is that capitalism does what capitalism does best:
It cuts costs.
- More patients to nurse ratio (Simply unsafe given most medical professionals already lack sleep)
- Little to no compensation relief on the way. (Huge boom of travel nursing during pandemic)
- Excess job responsibilities (More paperwork/aid duties, less actual nursing)
- New talent / old talent challenges (Larger incentive to switch jobs, hard to properly train)
We better figure out something soon. The medical field feels like it's holding on by a thread. Insurance companies run rampant with no end in sight. Health care continues to increase in costs and fail patients to the point of walking out or even dying to get care.
While I think generally speaking, nurses like my sister just want to feel appreciated like other jobs people are burning out in. You can do that in many different ways:
- Don't overwork them.
- Don't underpay them.
- Don't give them unwanted responsibilities.
- Most importantly, listen to them.
I think you may find that people actually do love the profession as it's one of the most noble professions out there, just that they are being forced out of doing something they love because of greed. Greed is not good.
The tragic insertion of a middle layer, the insurance industry (AKA Death Panels), makes it even more tragic and inefficient.
You can not seek profits in a competitive environment without reducing every cost to the bare minimum. Of course they are going to cut staff costs, and the number of properly staffed beds to the bare minimum, it minimizes costs. If a surge happens, they're happy to pay a little bit of a premium in the cost side for extra staffing. It's more than compensated by the extra billing.
But the recent public health emergency was a seiche, a tsunami, a pulse of unanticipated magnitude. (Unanticipated in the minds of those looking to meet this quarter's numbers, not in the minds of long term strategic thinkers).
The wrong type of people are in charge of health care in the US, and our nation will not be secure until this changes.
Her most recent gig was in Antarctica. I mean, cool, right?
And why is it so hard to find the raw data from the actual survey? I'm surprised this is scoring so well on HN.
[0] https://www.hospiq.com/about-us/press-releases/new-hospital-...
So much sacrifice for the greater good, we the public are not worth it.
Another profession I always think of are math teachers, they are good people.
And no, "excellent work ethic" isn't enough.
In the same way that national defense has been driven into a profit making venture (and encouraging the support for proxy wars), health care has become a beast beyond monopolistic power, able to drive demand for its own supply. The net result has been to give responsibility without authority to the providers. Nurses are subject to mandatory overtime. Physicians are required to take unreimbursed call. These services were once the hallmark of a devoted provider. Now they are exploited by a corporate profit seeking behemoth.
Patients now have such large deductibles that they prefer to pay me in cash for a negotiated lower price. No longer is health insurance actually insurance. It has become more of a coupon or in the language of today's generation, a groupon.
Even retirees who with Medicare only had to pay 20% of unreimbursed allowable expenses, have increasing burdens. The premium for part B (yes you have to pay for the part of Medicare that does not cover the hospital) has increased 15% this year and the government stated this is largely the result of a single dementia therapy - a pill that costs $56,000.
I think we could fix the problem if we required our lawmakers to actually pay for their healthcare. They get it for free. In addition, each gets a multimillion dollar stipend to run their office, separate and apart from their generous salary. For doing what? pushing emails. And they are so afraid of offending any part of their constituency that they spend most of their time arguing about non-issues. Their ridiculous behavior is creating a fertile environment for the next tyrant who will prromise salvation and deliver true misery.
the health of the patient became subordinate to the economic incentives of the hospitals and the other involved institutions (insurance providers, pharmaceutical corporations, etc...)
and so I have the hypothesis that this happened because people (young adults) going into medicine because of a vocation to help and heal others become disheartened when they find out it's all about institutional profit; only them who get into this becuase "doctors make good money" really make it to the end (which is not terrible, as they usually do learn the methods and techniques of medicine, but that in the long run prioritize money over health).
health care should have never been allowed to become a capitalist marketplace.
I can't even imagine what nurses have gone through being front line staff interacting with patients (and their families) all day. We need a zero-tolerance policy for families that verbally abuse front line staff, but instead they are often let off due to "stress of a family member in hospital" or the need for "family centered care".
[1] https://www.icn.ch/system/files/2021-07/ICN%20Policy%20Brief...
I'm trying to think of how any of those can be solved with "technology" :-/
Last year she retired from the profession entirely, a few years ahead of "normal retirement age", and now she works part-time at a local farm/fruit stand. The main things that drove her to retire early was management insisting on 12 hour shifts and not hiring enough staff.
And really, this is a red herring; the real problem started long before COVID. This video essay nails it (or so care practitioners at my workplace say, anyway): https://www.nytimes.com/video/opinion/100000008158650/covid-...
Ugggh, maybe it can't? As the main problems seem to be political, not tech related?
You might as well ask how IT can be used to fix homelessness or police brutality?
The nurses seemed excellent...but the amount of time and emotional energy they had to put into dealing with multiple computerized systems - just within my friend's room, to replace an empty IV bag - was staggering. The "smart" IV pump was the worst - a crappy little display, a minimized number of flaky buttons as the only interface, and the nurse had to drill down into multiple sub-sub-sub menu's to do even basic stuff.
My first thought was that you could triple nurse productivity (as in "care given to sick humans") if you had two IT tech's following each nurse around, tasked with doing all the "re-redundant data entry & dealing with computerized shit" that had obviously become the nurse's primary job.
My second thought was that interfaces which the nurse had to deal with should be restricted to 1950's-industrial-control-panel style - nothing but well-labeled, single-purpose physical buttons, switches, & dials. And the data entry that they had to do was restricted to wax pencils on well-laminated paper - which could be fed to a scanner, to update the patient records database. (Displays, say of vital signs & such, could be fancy. But the "50's control panel" rule could put an end to "oh, that information is hidden down in a sub-sub-sub-menu here..." shit.)
Second hand impression from a doctor friend.
This is pretty much universal in my experience. As a dev, it always seems to boil down to these. It's amazing how the business doesn't know their processes, can't document them accurately, or simply don't care to analyze and document them. Garbage requirements become a garbage system.
I have family members in medicine, and they see the same thing. There was a really good opportunity at that time to address some glaring issues with healthcare, and we ended up with this thing that did not address those issues and created a lot more issues.
The travel nurses make significantly more and now that she has basically hit her cap (after just four years) I've been trying to convince her to move to a different unit or get a different job
That is 0.00008 % of all RN's in the US.
Kind of weird that the usa prioritizes software developers over healthcare workers in the immigration system .
Nursing educators aren't exactly a dime a dozen. The average age of a masters prepared nursing educator in the us ranges between 56-62. Doctorally prepared is higher. The country is facing a nursing shortage, and a nursing educator shortage.
Now my doctor has an interesting theory that some of the pain points for nurses is being created by the hospital systems and industry themselves as an excuse to say we dont have enough nurses and bring in nurses from other countries like the Philippines, as they'll be glad to come to the US and work for less, and will be so grateful for the opportunity that they'll go along with whatever the hospital says they need to do. (This was in the context of vaccines.)
The other thing that has nurses worked up is recently is this case: https://www.cbsnews.com/news/radonda-vaught-nurse-guilty-dea...
What a shitshow.
Then if they work for years they might increase in pay band from like 2 to 4 which takes them up to like 20k-22k
Absolute joke for the hard work they do
Just kidding. Teachers used to almost all be male until public schooling and the resultant budgeting turned them female (to pay them less.) It's like reverse computer-programming where the profession turned male when they started paying more.
Pay them and they won't leave. Pay them a lot, and dudes will start writing essays about how the reason women aren't being hired and are leaving the profession is because they naturally have less of an interest and aptitude for nursing than males.
(I have a nurse in my family)
Lots of considering leaving a profession, also considering losing fat on Jan 1, and saving for retirement.
When people are surveyed there is a big difference between why they say and why they actually are doing the action. For example "Yeah, covid has been tough... and those insurance companies though... And doctors really dont respect my profession... Oh my [pregnancy/parental leave/dream of being a DJ]? yeah that has nothing to do with it."
These kinds of opinion surveys are just barely "science" .
- Nurses were getting burned out before the pandemic, and the US has a nursing shortage that's been going on for about 90 years (it started with an infrastructure buildout in the 1930s).* So it's a secular problem, with chronic as well as acute causal factors.
- There is a ladder of nursing credentials, and the shortage effects them differently. Hiring for roles like CNA and LPN/LVN has exploded because of the shortage of RNs and above. CNAs get trained in 4-12 weeks to do the heavy lifting of care; RNs get ~3 year degrees to perform much more complicated tasks.
- Burnout, and the nursing shortage, are in a positive feedback loop/downward spiral. That is, the more nurses burn out, the more they cause other nurses to burn out. Short-staffed facilities have a very hard time pulling back to normal staffing, because nobody wants to join a skeleton crew. (I know of long-term care facilities where the scheduling nurses (the bosses) are working the graveyard shift because they can't fill it.)
- Many nurses work rigid schedules on 12-14 shifts, and a lot of medical errors happen at the end of those shifts. **
- The hot US job market (Great resignation, great reshuffle) is hitting nursing especially hard; it is very sensitive to external shocks. There are paths to easier work and higher pay.
- Many healthcare facilities and systems don't give nurses flexibility or the possibility of advancement. (One family member will need to quit her current job and come back in a year or two to her current employer if she wants to move up a pay grade -- which is like some tech companies -- but slower moving and lower paying.)
- Many facilities are run entirely on foreign staff (the H2-B visa allows that). And many nurses are imported from the Philippines.
* https://www.nursing.upenn.edu/nhhc/workforce-issues/where-di...
** https://www.nytimes.com/video/opinion/100000008158650/covid-...
(plug: if you're interested in this problem, we're hiring: https://culture.clipboardhealth.com)
small sample size but agree on most points
Few people have been as relentlessly toxic and unforgiving on social media as nurses.
As a child of a nurse, that job has sucked for at least the past 40 years. The pay is average. Workplace is a cesspool of gossip and toxic work culture. Management is generally terrible. Also, the pandemic has exposed how many in the profession really are just narcissists.
The amount of facebook posts from indignant nurses spreading the most horrible comments , just to receive likes and be perceived as heroes, these past two years have made my stomach turn.
Its about time we cleaned up in healthcare. Not just aduquate pay, making sure we properly manage healthcare professionals and evolve healthcare management to grow where its needed.
I am 100% positive a flexible healthcare system that expands and shrinks after societal need is possible.
Not this crazy old fashioned fixed set of beds for x or y, that gets cut in some wave when they are needed less. Only to cause havoc in years when they are needed more.
Make sure the good nurses dont burn out and quit leaving the narcissist and ego maniacs behind.
There are amazing nurses out there, but we need to face that many of them are absolute shit at their jobs. And should seek other venues. This exodus may be a good thing in the end.
Hrmmm. Pretty sure if 90% of nurses actually left the profession it would be a serious problem.
That being said, I would be surprised if this actually happened. If even 5% left the profession would probably become more lucrative, since pay would have to rise to retain those who remain. Meanwhile, although nursing is not super highly compensated, the alternatives for someone who has only a nursing education and skillset will likely be worse. That may lead to a gap in ideation about leaving vs actually leaving, because the fact of the matter is that we all still have to put food on the table.
Saddest thing is that I really felt I was helping, but have to admit I've become burnt out in the healthcare field - Just have $500 or so in scrubs invested...
Taking the time has hurt my career in many ways, I do believe. I have a ton of respect for many nurses, but many travelers are worse than you might imagine. Over-extended, far over-paid for their work. And really don't care about the facility they are working with (or throwing others under the bus to cover up their own mistakes)...
It was a valuable thing to experience, and I do believe I helped many people, but it's a very different thing to be at the bottom rung than the one designing and implementing various systems. God forbid someone can see a workflow issue, propose multiple solutions, and have travelers ignore it because the workflow issue makes them more money.
Not a rant against nurses at all - As someone with over 20 years in various roles of engineering, it was quite an eye opener to me.
The issue with entitled, mean patients strikes me. While I'm sure a fair bit of this is due to the way in which misinformation about COVID and other health issues spreads on social media, I have a hard time believing this is the primary cause of this grumpiness. It seems more likely that the average person is just fed up being taken to town by a completely inhumane system that really ought to be the most humane of systems. Nurses are the front line representatives of a system that exploits people when they are most vulnerable.
Now, I'm not saying nurses deserve this at all. They're not to blame for the state of things. But the observation might go some ways in explaining the psychology of the phenomenon.
Source: Got nurses in the family.
In my opinion nurse should have shorter 8 hrs shifts and 4 per week . In this capitalistic driven health care system, where being a patient and health care provider comes with a cost.
It cost something like 15% of the nursing workforce, people who were already Covid immune, since they had worked the Covid front lines from day one.
But we pretended the vaccine helped stop the spread of Covid. It doesn't. And we pretended the vaccine had no meaningful risks. It does. And we pretended that natural (recovery) immunity didn't exist. It not only exists, but it's far stronger than anything a vaccine can do.
And yet we pretended anyway. And now we're paying the price. Pretending makes for bad public policy.
There are a lot of things we need to stop pretending about.
1. Everyone pays lip service. People stand at airports and say thank you for your service the same way they open their windows at 7PM and start clapping and cheering during shift turnover. Sometimes they'll say they know people who are veterans or 'frontline healthcare workers' as a sign of solidarity
2. Nobody actually wants to hear what you went through. Hearing people die or knowing people are about to die in sometimes painful, unfortunate ways is too raw for people to try to seek out and understand, despite the fact that for a significant portion of the population that's how we're going to go out, in a hospital with all sorts of drugs pumped into our system
3. There's a constant barrage of emotional/mental harm. Believe it or not, you don't magically 'harden up' immediately. Absorbing/witnessing drastic outcomes gets easier, but the burden doesn't get lighter. This isn't to mention physical harm. People do all sorts of things out of desperation and frustration.
4. The systems that manage you are byzantine if not kafkaesque. You're never sure how the decisions are made, yet you're the one that will be paying the most for it. You know deep down that you're just a number on a spreadsheet, and the only reason that keeps you going is internal motivation to do what you think is right, so you push on
5. The people who can help rarely think about you. Very few politicians will mention your name or your union that is doing its best to get some kind of safe nurse:patient ratios or even get the hospital to pay for your scrubs that they mandate. Very few billionaires have mentioned healthcare workers or veterans at all. As a whole, until someone has an emergency that threatens their physical or financial status, healthcare and security is treated as a black box with unreal expectations and extra sensitivity to deviations from said expectations, despite a complete lack of introspection and information on how those expectations came to be
I don't know what the solution is. In healthcare, every system is so deeply connected to the rest that destroying one or even refactoring takes down everything else, and we need it to stay online. The same applies to the continuation of geopolitics by other means. You can give every IC the best EMR system, the best rifle and radio, the best monitor/laptop/keyboard, but it's all for nothing if the system as a whole is a dumpster fire. Her frustration is palpable every time she finishes a rough shift (probably 2 out of 3), and the best I can do is lend my ear and pour a glass of wine.
That being said, I am grateful that she is continuing on the path. Our shared experiences have brought us closer than ever.
https://www.beckershospitalreview.com/workforce/if-1-in-5-he...
Now, the problem is that when people started quitting, there were fewer nurses to take care of the patients and their ratios went up. During normal times, a floor nurse might be 6-8 patients to one nurse, a step down unit might be 4-1, and an ICU might be 1-1 or 1-2. It depends on the level of care required. Now, they're doing more than double this on a regular basis. And, frankly, they can't do it, at least safely. There's a number that a nurse can call if they believe they have an unsafe number of patients in order to get some kind of legal protection, but they still have to see that number of patients. And, frankly, it's incredibly stressful because they really, truly can't take care of that many patients, so they quit. A friend of my wife is a nurse trainer at a large hospital. They're having 80% of new nurses quit during their onboarding process because the ratios are absurd. A good portion of my wife's time is spent figuring out who's the least sick patient to discharge from the ICU because they don't have the staff.
Unfortunately, I don't think we're even close for this to being over either. The constant refrain is that COVID is the new normal and we need to adjust. I would contend that a new normal would imply a stable operating point and I do not believe this to be the case. It's going to take a really long time to restaff appropriately where the patient ratios and stress level manageable. Long time means years because, really, hospitals want and need BSNs and not just associates level training. In the mean time, every time we have a COVID surge, the hospital gets flooded, everyone gets overworked and abused, and more people quit.
I think your would be headline is a fair inference to come to, though not the sole cause.
With how over sensationalised our media is, can we avoid complaining when headlines actually directly match the thing they're reporting on for once?
One fundamental force in nursing is that a nursing shift is unpredictable. Some shifts go very smoothly, some are absolute trainwrecks. Patients are, definitionally, sick enough to be in a hospital, and they can start declining very quickly. This means that whatever you are doing at any given moment is often interrupted by a new priority that must be handled RIGHT NOW. It means that your 'plan of attack' for the day (which patients get [meds | baths | food | mobility | turns | dressing changes] when) is often delayed, sometimes by several hours. Any number of things could push the schedule back - incontinence care, a doctor stopping by to discuss a patient with you, a patient fall, a medical emergency, a lonely patient. A few curveballs can put you way into the weeds.
Consequently, the culture on a floor is key to how good your shift is gonna be. If you help others out when you have some slack and they help you out in turn when you are behind, it really smooths out those rough days. If other nurses let you drown, you drown.
The biggest thing that a hospital can do to help nurses is to adequately staff their floors. If everyone is drowning because the floor is understaffed, no one has time to help each other. If you're caring for six patients instead of four (on a med-surge floor), there are days where there literally isn't enough time to do all the nursing care everyone deserves. Documentation can be, and often is, done after passing off your patients in report. After you've already "dropped" documentation from your during-shift schedule, patient mobility - getting people up and walking, or even just sitting up in a chair for meals - is the usually the next thing go. After that, hygiene. Nobody dies if they don't get a bath, but another patient certainly could die if you don't do X. Next up comes pain medication requests and incontinence care. For me, it was enormously stressful not being able to provide the quality of care that the patients deserve.
This can be a huge factor in burnout. The pandemic made things worse in a bunch of different ways. Besides the stress of caring for patients with a deadly virus, you also now have to add on several minutes to every patient interaction for donning and doffing PPE. That's even less time to do the nursing part of the job while you're dealing with a more critical patient population (who will need more care). Burnout rates increase and nurses leave, either leaving the profession or taking contracts that, even if the conditions are no better or much worse), at least pay a premium. Hospitals that were well-staffed face staffing shortages, and hospitals that were already short on staff are now in a staffing crisis. The hospitals have to spring for travel contracts, and the nurses that did stay are angrier that other nurses are making multiples of their pay for doing the same work.
Given that this thread has some 900+ comments already, this comment will start off pretty far down the list. But I see some people mentioning that you are working on trying to make things better for nurses - I'm guessing that those people will read the thread more thoroughly. I would love to chat with you about whatever it is that your startup / company / weekend hackathon project is doing in this space. I've dedicated five years of my life to the problem space and would happily share my thoughts and experiences.
It's unsurprising that what has happened in the past couple of years is putting stress on a system with the slack pulled out of it.
What's worse is it belies an ugly aspect of human nature (particularly pervasive in the US IME) that people absolutely do not give a fuck about anyone else when it comes down to it. As long as someone is fortunate enough to have decent health insurance through their job, people who don't are lazy.
The big picture here is that the wealthy want people dependent on jobs and to be in debt (eg student debt) because it makes them compliant.
So I'm not surprised nurses are leaving. Insurance companies make providing healthcare an absolutely miserable business and deliberately killing people ("prior authorizations", "pre-existing conditions", etc) should not be the basis for commercial enterprise. Denying someone life-saving or life-changing care should not be a profit motive.
What's worse is that a lot of the burnout is effectively caused by people who are profoundly selfish and are voluntarily choosing to get sick and die of what is now a highly preventible disease.
It's a hard situation because people depend on nurses so collectively they're torn. Teachers OTOH aren't life-critical (but still obviously important) so I'd actually like to see them make a mass exodus over all the right-wing censorship they're facing in most states.
You can do almost any job with almost any degree.
Salary for nurses varies widely, and in some places, they're wage-competitive with Amazon delivery drivers now. I can easily see people deciding that even though they like helping folks, getting paid less than the people who drive around and drop packages all day doesn't seem like a fair deal.
It sounds like they're just being overworked. So, just have the nurses take a 20 minute break every 2 hours, to go out and take a walk. The hospital can require it if it comes to that but why wouldn't they just want to do it? and if the hospital doesn't want to do it, then the nurses should insist on it and walk off the job if not given their breaks. I would imagine the hospital would rather agree to 20 min breaks every 2 hours rather than loosing 90% of their workforce forever: they don't have a choice, they have to agree.
Registered Nurse (RN): The 'specialized nurses' you talk of, and what this article is mainly about. Requires at least an associate's degree to be licensed, but increasingly an bachelor's is expected. Only they can administer any medication a doctor prescribes, and only they can assess your condition.
Licensed Practical Nurse (LPN): If they are certified they can also do blood draws. Requires graduation from an LPN program (usually about one year) to be licensed. They perform easily predicted tasks like a dressing change that do not require assessment. They can also administer some drugs based on the situation.
Unlicensed Assistive Personnel (UAP): In a big hospital, these are who are checking your temperature most of the time. They can only do basic tasks that do not require any medical training, even if their experience is larger than the RNs and LPNs they're under.
There are also many different technicians. In a big hospital, an RN acts as a middle manager delegating their work to these many different tiers. In an ICU, or in a small hospital, it will be done much more by themselves.
There's just something masochist about their profession.
It'd also be enlightening for people in this thread to have hospital executives explain how they have some of the highest patient numbers in history yet they're hemorrhaging so much money their physicians had to take pay cuts.
Nurses, due to their profession having relatively low barriers to entry yet requiring years of operational knowledge to truly be effective, need collective bargaining. Nurses do strike, and nurse strikes are actively occurring on the U.S. West Coast. However, the unions they represent are small and have little power overall. For a strike to be successful you need solidarity from a majority of workers in the area you want to impact. You also need buy-in from the hospital/region that union nurses will provide superior care to non-union nurses. Something that's hard to do when your average executive thinks that the most complicated thing a nurse does is sticking a patient.
It's not about the illegality, it's really just about people dying. Yes you can go on a strike but your patient that's in critical condition won't survive on principle. You could say "just don't care about the patient and strike anyway", but that's extremely hard to do.
Striking when it hurts some millionaire owner is one thing, you wouldn't feel bad about yourself. Striking when it hurts someone post-op who did nothing wrong aside from being sick isn't noble, you get to live with the fact that as an individual you could have saved them, yet you didn't because you wanted money.
Not a chance, not a speculation, but absolute awareness of the number of patients that will not receive care and likewise will die as a result.
I don’t think it’s fair to blame nurses for poor treatment when they have a multitude of terrible options to pursue in order to improve their working conditions.
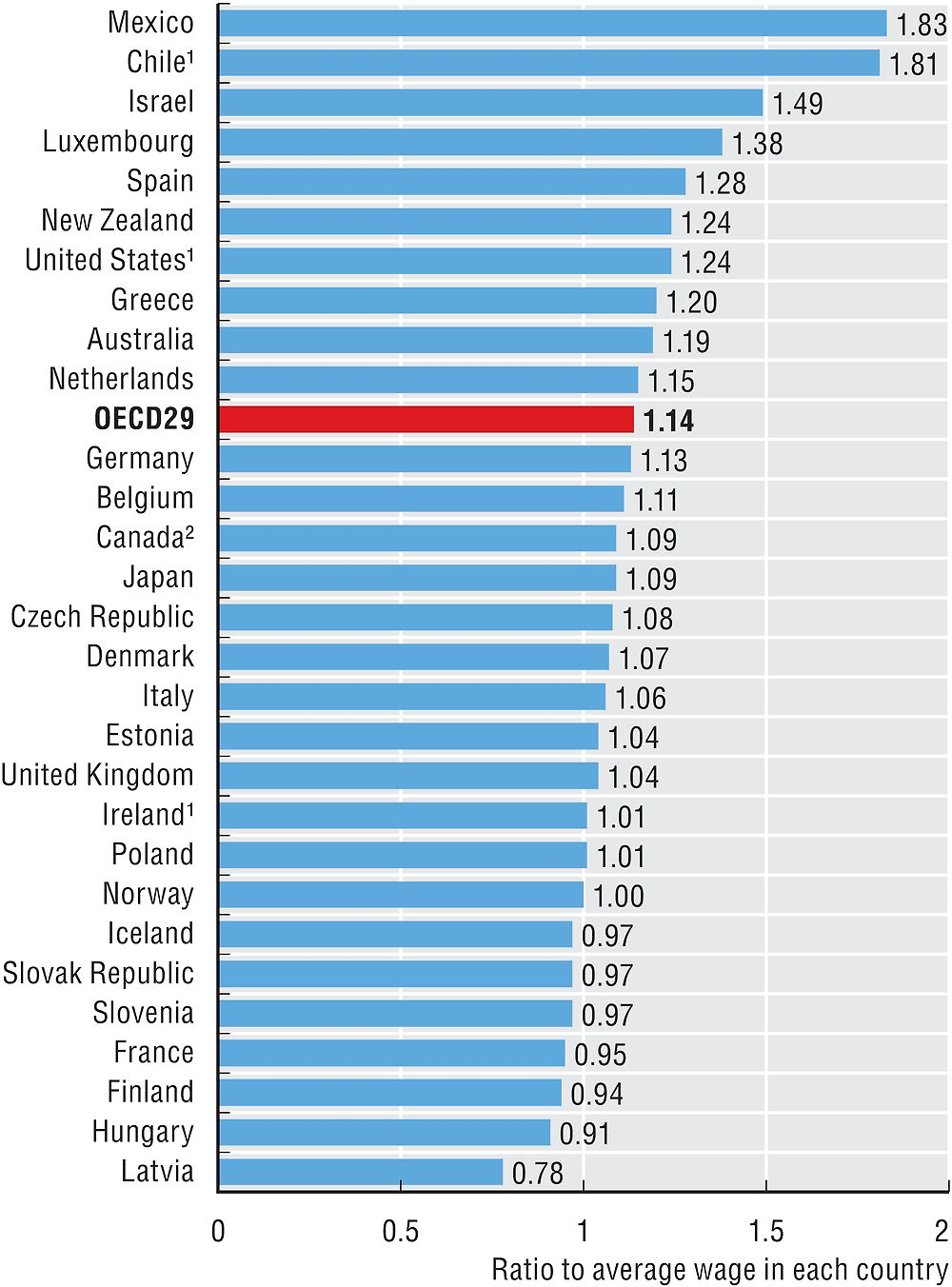{kind=link}
{kind=link}
{kind=link}